Both of them could be weakened by direct trauma 12 17 ischemia so called.
Diplopia downgaze after orbital floor repair.
This video illustrates the use of porous polyethylene implant stabilized with cyanoacrylate glue to repair an orbital floor fracture by the transconjunctival technique in a 10 year old child who had sustained a facial trauma.
Cho who determined that the patient probably had not needed the orbital floor fracture repair in the first place.
Diplopia in patients with orbital floor fractures may appear in either up or downgaze or both 9 14 the etiology of this phenomenon has been speculated on since lerman s 1970 study.
Endoscopic repair of the orbital floor blowout fracture using an endonasal approach appears to be a safe and effective technique for the treatment of diplopia.
Finally after attempting two revisions the surgeon referred the patient to dr.
After the initial surgery the patient had diplopia hyperglobus and cicatricial entropion.
Orbital blowout fracture od s p repair with orif and placement of a plate 7 weeks prior.
We retrospectively studied 54 patients who underwent repair of an orbital blowout fracture.
Double vision after orbital floor repair unread post by moby thu sep 17 2009 10 16 pm hello and welcome i am sorry to hear about this serious injury.
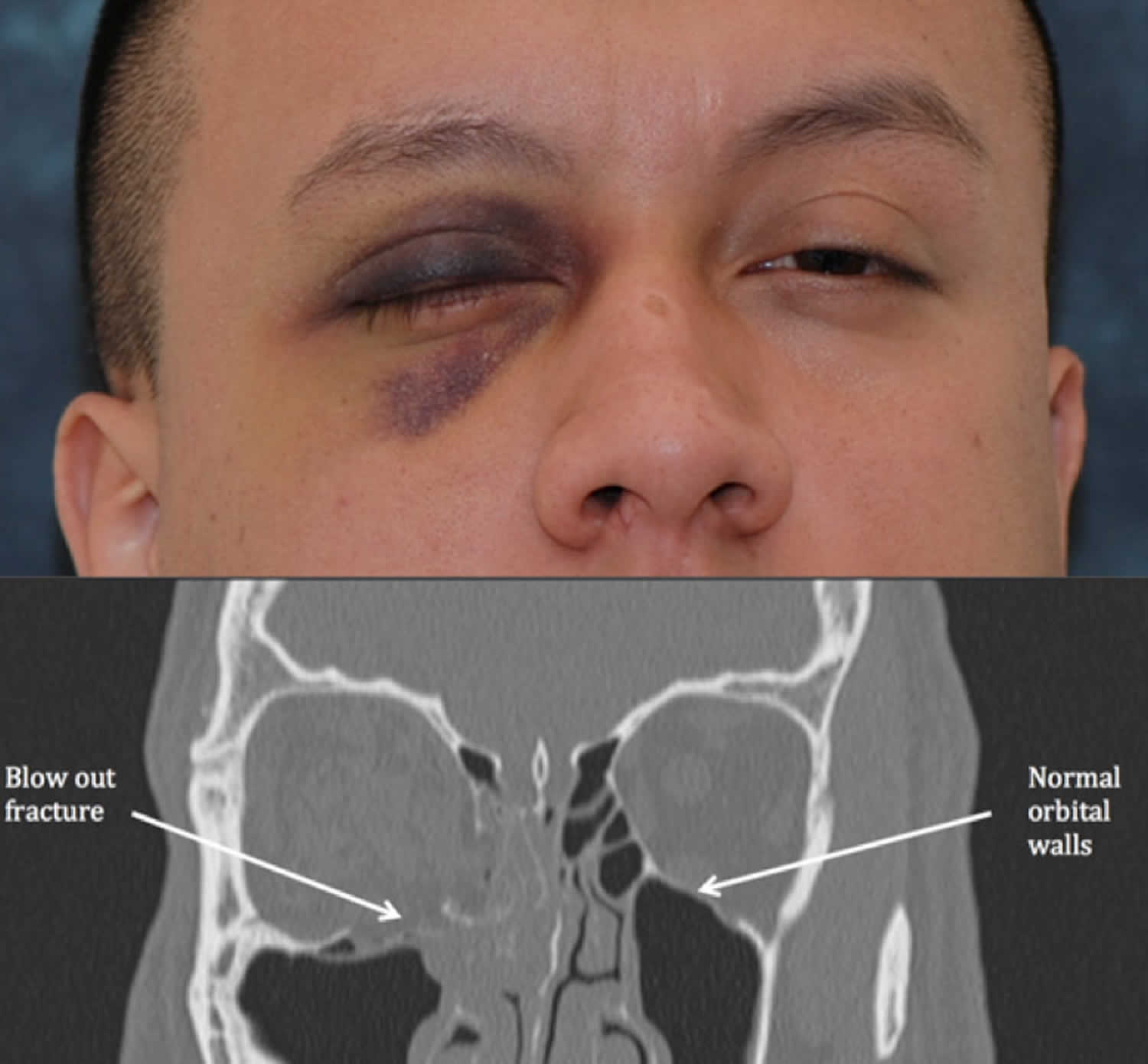
The eye may be proptotic or enophthalmic depending on the amount of edema causing proptosis and the size of the fracture larger fractures leading to enophthalmos.
16 the inferior rectus muscle and the inferior oblique muscle may be involved.
Immediately after an orbital floor fracture the affected eye may have impaired motility resulting in double vision.
Persistent diplopia has commonly been reported as a complication of orbital floor fracture repair in children.
1 2 in patients with postoperative diplopia restricted extraocular motility and positive forced ductions surgical exploration for residual inferior rectus entrapment is indicated.
A total of 47 of 54 86 patients had clinically significant diplopia.
This technique has many advantages including simplicity of continue reading.
She had an incarcerated inferior rectus muscle in the fracture causing diplopia in upgaze.
Two patients with posterior fractures showed persistent diplopia which was well managed by prisms.
A minimum of 6 months follow up was available for all patients included in the study.
However here we present two cases of marked upgaze limitation and positive forced ductions 1 week.
None of the patients reported diplopia in the primary position neither downgaze conclusion diplopia persisting after reconstructive surgery of a fractured orbital floor may be corrected surgically.